Epstein syndrome is a hereditary disease characterized by 3 symptoms: 1) macrothrombocytopenia, 2) progressive renal dysfunction, and 3) sensorineural hearing loss. As for 1) macrothrombocytopenia, giant platelets are observed in blood tests in all patients with Epstein syndrome since birth. In some patients, the finding of macrothrombocytopenia leads to an early diagnosis of Epstein syndrome. On the other hand, the time of onset of 2) progressive renal dysfunction and 3) sensorineural hearing loss varies among patients. In patients who develop renal dysfunction at an early age, proteinuria and hematuria are observed in urinalysis since around the age of 5 to 13 years, and kidney function decreases with increase of proteinuria in the late teens or later. In patients whose kidney function decreases at an early age, hearing loss also appears at the same time as proteinuria and progresses with increase of proteinuria.
Patients with Epstein syndrome have the 3 symptoms below:
1) Macrothrombocytopenia
2) Progressive renal dysfunction
3) Sensorineural hearing loss (high tone)
There are also rare cases of cataract. Details of each symptom are described in the following paragraphs.
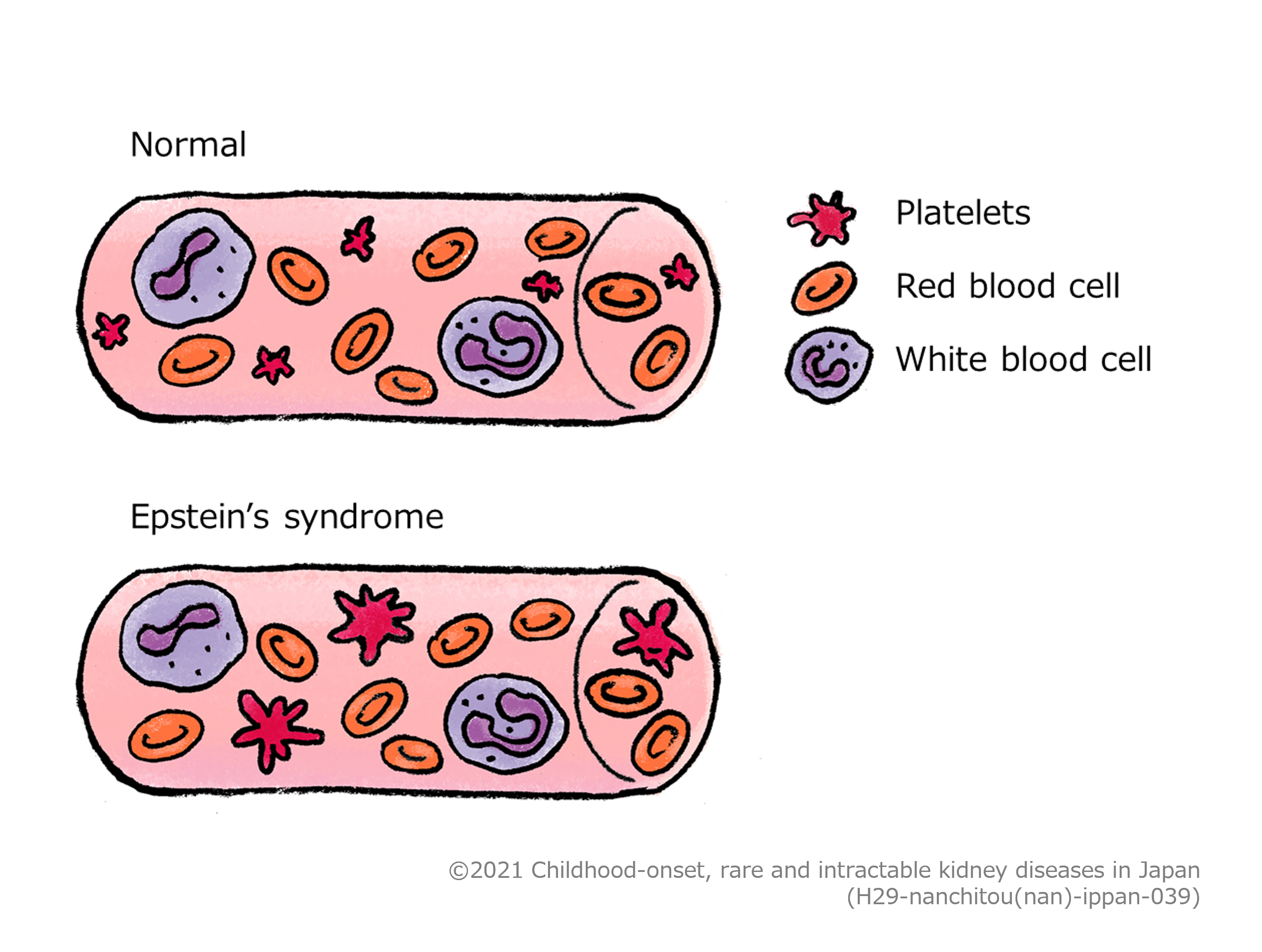
The function of platelets is to adhere to the site of blood vessel injury and close the hole in the blood vessel. The number of platelets in the blood in a healthy person is about 150,000 to 400,000/μL, whereas in patients with Epstein syndrome, the number is about 20,000 to a few tens of thousands/μL or less (a few thousands/μL). Therefore, when these patients get injured or undergo surgery, it is difficult to stop bleeding. Patients with Epstein syndrome may be diagnosed by bleeding tendency due to thrombocytopenia in infancy or later. Many patients are diagnosed with another disease associated with decreased platelets and receive treatment to suppress the immune function. In patients with Epstein syndrome, not only is the platelet count low, but platelets are also large (giant platelets), and this feature often leads to a diagnosis of Epstein syndrome. Patients with Epstein syndrome rarely have serious bleeding even if the platelet count is very low. However, because it is a fact that these patients are bleed easily, extra caution should be paid especially to intracranial hemorrhage due to head trauma. Platelet transfusion may be required before surgery.
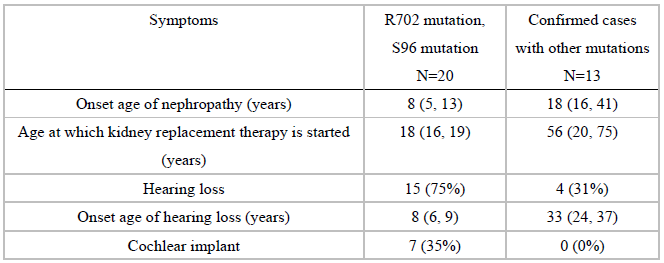
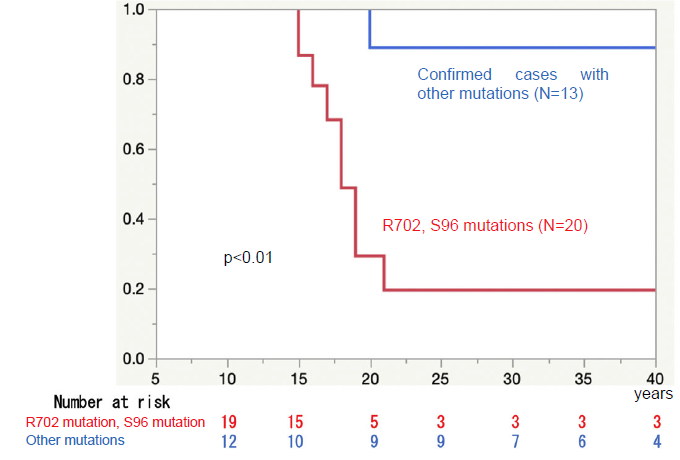
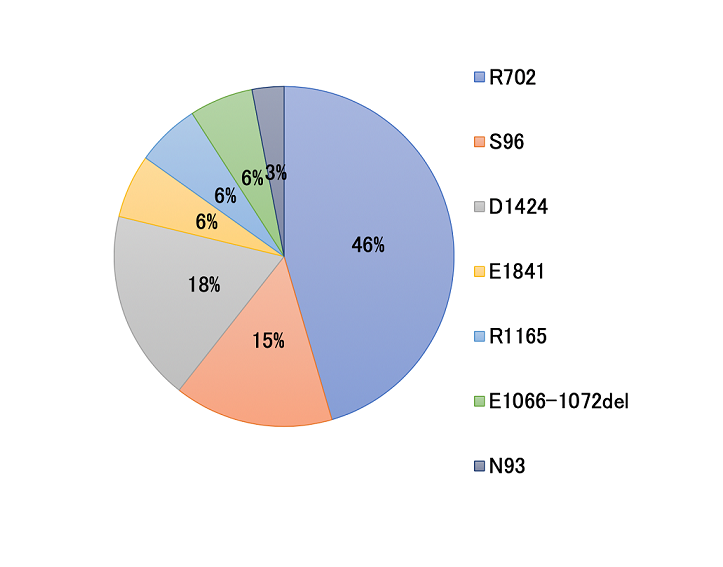
The most problematic symptom for patients with Epstein syndrome is progressive renal dysfunction. It is said that patients with specific types of gene mutations associated with fast progression of the condition (R702 mutation, S96 mutation) typically have urinalysis abnormalities, mainly proteinuria, at around the age of 5 to 13 years, followed by the deterioration of kidney function starting relatively early, and are likely to progress to end-stage kidney disease (condition requiring dialysis or kidney transplantation) around the age of 20 years. With other types of gene mutations, the speed of progression of renal dysfunction is varied among patients. It may be possible to decrease proteinuria and delay the progress of renal dysfunction by starting to take medicines to regulate blood pressure (angiotensin receptor blocker) at an early stage, but the effect is still unclear. Dialysis and kidney transplantation require surgery, but these interventions can be performed safely with platelet transfusion.

The severity of hearing loss is considered almost in proportion to that of renal dysfunction (patients with severe renal dysfunction have severe hearing loss, and in contrary to this, patients with mild renal dysfunction have mild hearing loss). Like other cases of hereditary hearing loss, the type of hearing loss observed in Epstein syndrome is high-tone hearing loss (also known as sensorineural hearing loss), in which high-tone sounds (6000 to 8000 Hz) are harder to hear. The ability to hear the low to middle frequency range is maintained relatively well, and so even if high-tone hearing loss considerably progresses, patients can hear sounds to some extent without using a hearing aid. The severity of hearing loss needs to be measured accurately by using a test method called an audiogram at an otolaryngology clinic. If necessary, patients use a hearing aid or undergo cochlear implant surgery.
Like many other hereditary diseases, there is currently no curative fundamental treatment for Epstein
syndrome. Epstein syndrome is associated with the three above-mentioned main symptoms.
As for thrombocytopenia, platelet transfusion may be given before surgery, but in everyday life, the only
thing necessary is to be careful to avoid head trauma (intracranial hemorrhage), and no specific treatment is
needed.
Regarding progressive renal dysfunction, it may be effective to use blood pressure-lowering medicines
classified as angiotensin receptor blockers when proteinuria appears because these medicines possibly delay
the progress of renal dysfunction. However, even with this treatment, most patients with specific types of
gene mutations associated with fast progression of the condition will require dialysis therapy or
transplantation therapy. Dialysis (hemodialysis or peritoneal dialysis) and kidney transplantation are
performed safely in most patients with Epstein syndrome by paying due attention to bleeding tendency.
As for sensorineural hearing loss, patients are advised to undergo audiometry periodically and, if necessary,
use a hearing aid or undergo cochlear implant surgery.
Little had been known about Epstein syndrome until the causative gene was identified after the year 2000, and there had been many cases incorrectly diagnosed as other diseases (e.g., idiopathic thrombocytopenic purpura, Alport’s syndrome). The precise number of patients in Japan is unknown. Based on a survey, the estimated number of patients in Japan is around 200. As this disease becomes better known in the future, more patients may be identified.
It is obvious that Epstein syndrome is a hereditary disease. The symptoms appear due to congenital abnormalities of the molecules that give shape to the cell and maintain it in platelet-producing cells, kidney cells, and sound-sensing cells in the ear. This molecule is called non-muscle myosin heavy chain IIA. There are various types of myosin molecules; they have motor function in the muscle, whereas non-muscle myosin heavy chain IIA has the function of shaping cells in non-muscle cells. Because of this function, non-muscle myosin heavy chain IIA is called the cytoskeleton molecule . In Epstein’s syndrome, congenital abnormalities in the gene called MYH9, which functions as a blueprint of non-muscle myosin heavy chain IIA, cause abnormalities of platelets, kidneys, and ears in which non-muscle myosin heavy chain IIA plays an important role.
It is clear that this disease is hereditary. The mode of inheritance for this disease is autosomal dominant. In autosomal dominant inheritance, an affected parent, either male or female, has a 50% (1/2) chance of passing the disease on to a child. However, there are also many cases where a child born to parents with no abnormalities has a de novo mutation and develops the disease. In this case, when the child grows up and becomes a parent, his/her child has a 50% (1/2) chance of inheriting the disease.
The condition of thrombocytopenia does not change throughout life. There is no threat to life if major bleeding is avoided, and platelet transfusion is given as necessary in unavoidable situations such as surgery. On the other hand, for patients in whom proteinuria appears and renal dysfunction may progress, angiotensin receptor blockers may delay the progression of disease. However, if renal dysfunction still progresses to end-stage kidney disease, the patient needs to undergo dialysis (hemodialysis or peritoneal dialysis) or kidney transplantation. It is becoming known that most patients with specific types of gene mutations associated with the fast progression of renal dysfunction (R702 mutation, S96 mutation) require dialysis or kidney transplantation at around the age of 20 years. In Japan, as dialysis and kidney transplantation are performed without problems in patients with Epstein syndrome, these treatments are available at an appropriate medical institution. Hearing loss generally progresses in proportion to the progression of renal dysfunction. If the condition worsens, and the use of hearing aids becomes insufficient, the patient may undergo cochlear implant surgery. As described above, although renal dysfunction and hearing loss progress in Epstein syndrome, there are drug therapies that may delay the progression of renal dysfunction and ultimately, kidney replacement therapies such as dialysis and transplantation. Therefore, the most important thing is to consult closely with the attending physician.
As for thrombocytopenia, strict precautions are not necessary, but major bleeding should be avoided. More specifically, any sport or play involving fierce physical contact is not recommended. Treatment of renal dysfunction is especially important. Please consult closely with your attending physician so that you can have your lifestyle and medications adapted to the severity of renal dysfunction. For example, salt restriction is necessary if you develop hypertension, while drug therapies are necessary if your kidney failure progresses.
Note: Macrothrombocytopenia is observed since birth, whereas 2 and 3 develop at the age of 5 years or later.
Definite: Criterion 1 of A and both criteria of B are met.
Any of Stage II or higher macrothrombocytopenia based on the severity classification for idiopathic thrombocytopenic purpura, severe or profound hearing loss, and kidney condition categorized as “Red” in the CKD severity classification heat map is considered as a designated intractable disease.
<Macrothrombocytopenia>
Stage II or higher based on the severity classification for idiopathic thrombocytopenic purpura (Table
1).
Table 1 Severity classification for idiopathic thrombocytopenic purpura
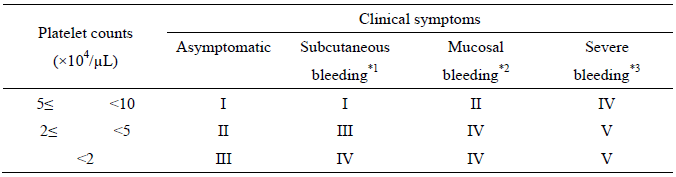 *1 Subcutaneous bleeding: spotting, bruising, ecchymosis
*1 Subcutaneous bleeding: spotting, bruising, ecchymosis
*2 Mucosal bleeding: gingival hemorrhage, epistaxis, melena, hematuria, hypermenorrhea, etc.
*3 Serious bleeding: possibly life-threatening cerebral hemorrhage, severe gastrointestinal hemorrhage,
etc.
<Sensorineural hearing loss>
Severe or profound hearing loss.

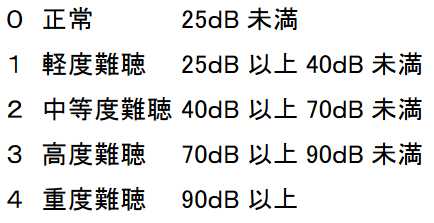
*Evaluated based on the mean values at 500 Hz, 1000 Hz, and 2000 Hz in the ear with better hearing (better-hearing ear).
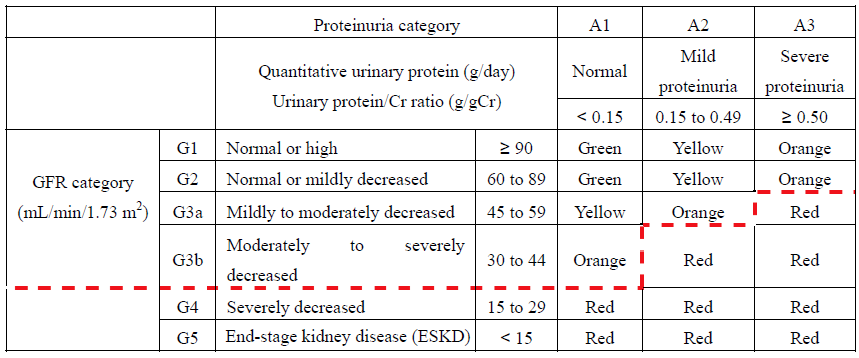
<Progressive renal dysfunction>
Condition categorized as “Red” in the CKD
severity classification heat map (Table 2).
Table 2 CKD severity classification heat map
Points to be considered when applying the diagnostic criteria
and severity classification
1. If there is no specific specification as per the diagnostic criteria, diagnosis can be made based on
clinical symptoms, laboratory findings, etc. observed at any time (limited to clinical symptoms, etc.
consistent with the clinical course of the disease and confirmable).
2. Severity classification after the initiation of treatment should be based on the worst condition, as
judged by the physician, in the last 6 months of treatment under appropriate medical management.
3. Patients in whom the severity of symptoms does not meet or exceed the specified level based on the above
severity classification but who need to continue expensive medical care are entitled to financial assistance
for medical expenses.